September 21, 2012 Medicare Bills Rise as Records Turn Electronic
By REED ABELSON, JULIE CRESWELL and GRIFFIN J. PALMER When the federal government began providing billions of dollars in incentives to push hospitals and physicians to use electronic medical and billing records, the goal was not only to improve efficiency and patient safety, but also to reduce health care costs.
But, in reality, the move to electronic health records may be contributing to billions of dollars in higher costs for Medicare, private insurers and patients by making it easier for hospitals and physicians to bill more for their services, whether or not they provide additional care. Hospitals received $1 billion more in Medicare reimbursements in 2010 than they did five years earlier, at least in part by changing the billing codes they assign to patients in emergency rooms, according to a New York Times analysis of Medicare data from the American Hospital Directory. Regulators say physicians have changed the way they bill for office visits similarly, increasing their payments by billions of dollars as well. The most aggressive billing -- by just 1,700 of the more than 440,000 doctors in the country -- cost Medicare as much as $100 million in 2010 alone, federal regulators said in a recent report, [1] noting that the largest share of those doctors specialized in family practice, internal medicine and emergency care. For instance, the portion of patients that the emergency department at Faxton St. Luke's Healthcare in Utica, N.Y., claimed required the highest levels of treatment -- and thus higher reimbursements -- rose 43 percent in 2009. That was the same year the hospital began using electronic health records. The share of highest-paying claims at Baptist Hospital in Nashville climbed 82 percent in 2010, the year after it began using a software system for its emergency room records. In e-mailed statements, representatives for both hospitals said the increases reflected more accurate billing for services. Faxton also said its patients required more care than in past years. Over all, hospitals that received government incentives to adopt electronic records showed a 47 percent rise in Medicare payments at higher levels from 2006 to 2010, the latest year for which data are available, compared with a 32 percent rise in hospitals that have not received any government incentives, according to the analysis by The Times. The higher coding has captured the attention of federal and state regulators and private insurers like Aetna and Cigna. This spring, the Office of Inspector General for the federal Health and Human Services Department warned that the coding of evaluation services had been "vulnerable to fraud and abuse." Some experts blame a substantial share of the higher payments on the increasingly widespread use of electronic health record systems. Some of these programs can automatically generate detailed patient histories, or allow doctors to cut and paste the same examination findings for multiple patients -- a practice called cloning -- with the click of a button or the swipe of a finger on an iPad, making it appear that the physicians conducted more thorough exams than, perhaps, they did. Critics say the abuses are widespread. "It's like doping and bicycling," said Dr. Donald W. Simborg, who was the chairman of federal panels examining the potential for fraud with electronic systems. "Everybody knows it's going on." When Methodist Medical Center of Illinois in Peoria rolled out an electronic records system in 2006, Dr. Alan Gravett, a former emergency room physician, quickly expressed alarm. He said the new system prompted doctors to click a box that indicated a thorough review of patients' symptoms had taken place, even though the exams were rarely performed, while another function let doctors pull exam findings "from thin air" and include them in patients' records. In a whistle-blower lawsuit filed in 2007, Dr. Gravett contended that these techniques drove up Medicare reimbursement levels substantially. According to the lawsuit, Dr. Gravett was eventually fired for ordering too many tests. He says he was retaliated against for complaining about the new system. The Justice Department is weighing whether to join an amended suit in Federal District Court in Central Illinois. An independent analysis by The Times showed that Methodist's Medicare billings for the highest level of emergency care jumped from 50 percent of its emergency room Medicare claims in 2006 to more than 80 percent in 2010, making the 353-bed hospital one of the country's most frequent users of high-paying evaluation codes.
Methodist declined to comment on Dr. Gravett's allegations. But in an e-mailed statement, a spokesman said that not all of the hospital's billing was done electronically, that it followed professional coding guidelines and that its patients required more care than patients at other hospitals. Many hospitals and doctors say that the new systems allow them to better document the care they provide, justifying the higher payments they are receiving. Many doctors and hospitals were actually underbilling before they began keeping electronic records, said Dr. David J. Brailer, an early federal proponent of digitizing records and an official in the George W. Bush administration. But Dr. Brailer, who invests in health care companies, acknowledged that the use of electronic records "makes it faster and easier to be fraudulent." Both the Bush and Obama administrations have encouraged electronic records, arguing that they help doctors track patient care. When used properly, the records can help avoid duplicate tests and remind doctors about a possible diagnosis or treatment they had not considered. As part of the economic stimulus program in 2009, the Obama administration put into effect a Bush-era incentive program that provides tens of billions of dollars for physicians and hospitals that make the switch. But some critics say an unintended consequence is the ease with which doctors and hospitals can upcode -- industry parlance for seeking a higher rate of reimbursement than is justified. They say there is too little federal oversight of electronic records. A spokesman for the Health and Human Services Department, however, said electronic health records "can improve the quality of care, save lives and save money." Medicare, he added in an e-mailed statement, "has strong protections in place to prevent fraud and abuse of this technology that we're improving all the time." He also said Medicare had reduced improper payments in the last two years. In emergency rooms, which use special billing codes to indicate how much care a patient needs, hospitals have increased their claims for the two highest-paying categories to 54 percent of Medicare claims in 2010, from 40 percent in 2006, according to The Times's analysis of Medicare data. The Center for Public Integrity, a nonprofit investigative journalism group, recently released a similar analysis. [2] Some contractors handling Medicare claims have already alerted doctors to their concerns about billing practices. One contractor, National Government Services, recently warned doctors that it would refuse to pay them if they submitted "cloned documentation," while another, TrailBlazer Health Enterprises, found that 45 out of 100 claims from Texas and Oklahoma emergency-department doctors were paid in error. "Patterns of overcoding E.D. services were found with template-generated records," it said. The Office of Inspector General is studying the link between electronic records and billing. One sophisticated patient witnessed the overbilling firsthand. In early 2010, Robert Burleigh, a health care consultant, came to the emergency room of a Virginia hospital with a kidney stone. When he received the bill from the emergency room doctor, his medical record, produced electronically, reflected a complete physical exam that never happened, allowing the visit to be billed at the highest level, Mr. Burleigh said. The doctor indicated that he had examined Mr. Burleigh's lower extremities, but Mr. Burleigh said that he was wrapped in a blanket and that the doctor never even saw his legs. "No one would admit it," Mr. Burleigh said, "but the most logical explanation was he went to a menu and clicked standard exam," and the software filled in an examination of all of his systems. After he complained, the doctor's group reduced his bill. As software vendors race to sell their systems to physician groups and hospitals, many are straightforward in extolling the benefits of those systems in helping doctors increase their revenue. In an online demonstration, one vendor, Praxis EMR, promises that it "plays the level-of-service game on your behalf and beats them at their own game using their own rules." The system helps doctors remember what they did when they successfully billed for similar patients, and ensures that they do not forget to ask important questions or to perform necessary tests, said Dr. Richard Low, chief executive of Infor-Med Corporation, which developed Praxis. "The doctor can use a chart the way the pilot uses a checklist," he said. But others place much of the blame on the federal government for not providing more guidance. Dr. Simborg, for one, said he helped draft regulations in 2007 that would have prevented much of the abuse that now appears to be occurring. But because the government was eager to encourage doctors and hospitals to enter the electronic era, he said, those proposals have largely been ignored. "What's happening is just the problem we feared," he said. [1] https://oig.hhs.gov/oei/reports/oei-04-10-00180.pdf [2] http://www.publicintegrity.org/2012/09/20/10811/hospitals-grab-least-1-billion-extra-fees-emergency-room-visits A Sharp Rise in Medicare Payments
Since 2006, inflation-adjusted Medicare payments for emergency-room services have increased more quickly than hospital costs.
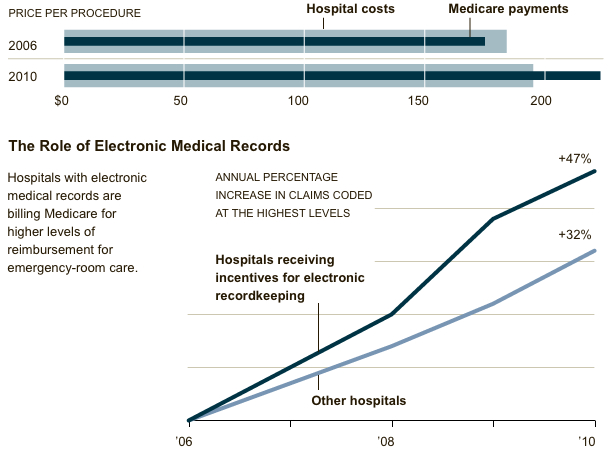
Source: New York Times analysis of Medicare data provided by American Hospital Directory